
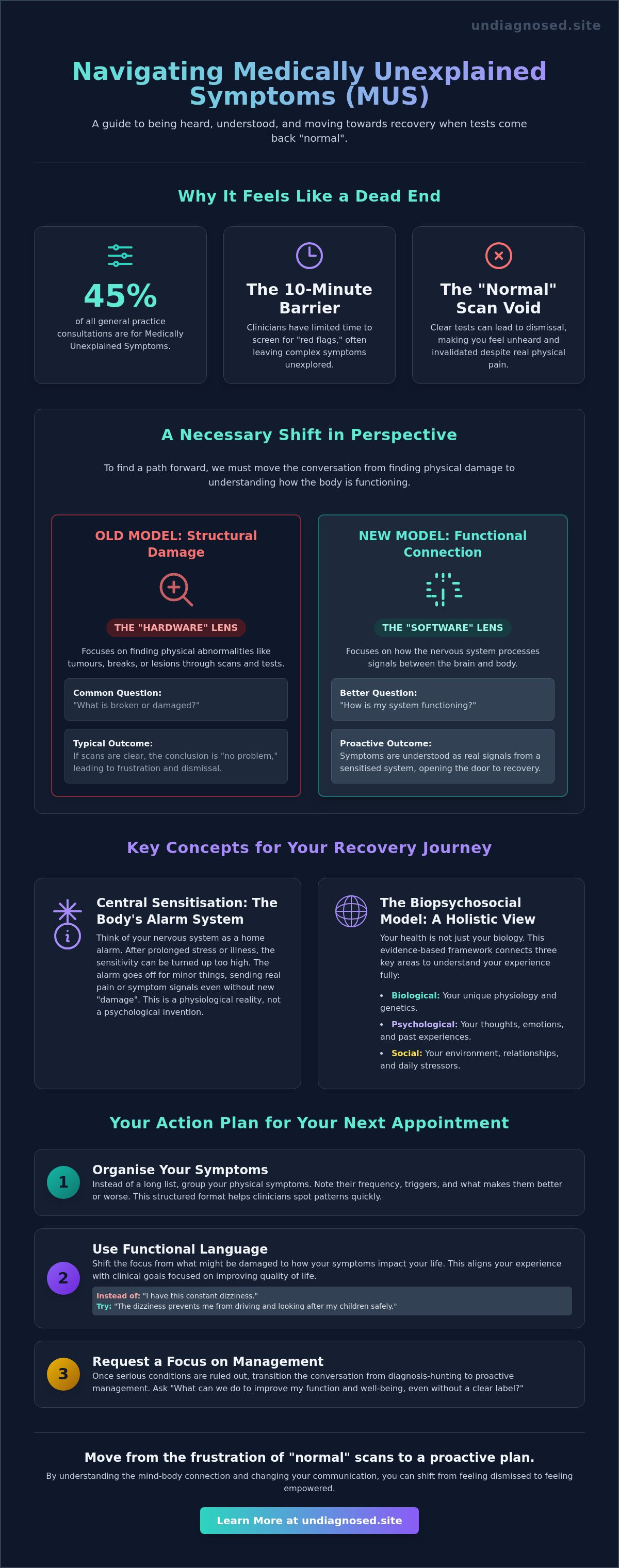
Did you know that Medically Unexplained Symptoms (MUS) account for approximately 45% of all general practice consultations? Despite representing nearly half of primary care visits, these experiences often leave patients feeling invisible. You likely know the exhaustion of clear scans and normal blood tests whilst your body continues to signal distress. It's frustrating to face the 10-minute GP appointment limit when your symptoms, from chronic pain to persistent dizziness, feel anything but brief. You aren't alone in the anxiety that a serious diagnosis is being missed simply because the current medical model lacks a label for your pain.
If you feel dismissed by the medical system, it's time for a different approach. This guide provides a framework for talking to doctors about MUS that shifts the focus from "finding damage" to "understanding function." We promise to show you how to ensure your physical experience is validated and understood, moving you toward hope, not hype. We'll explore a clear plan for your next appointment that bridges the gap between your mind and body through evidence-based guidance and practical communication tools.
Key Takeaways
- Understand the shift from structural damage to functional connection, moving beyond the binary of physical versus psychological illness.
- Learn to organise your physical symptoms into a structured format that helps clinicians identify patterns within the constraints of a short appointment.
- Master practical communication strategies for talking to doctors about MUS, using functional language to align your experience with clinical terminology.
- Discover how the neuroscience of the Mind and Body Connection provides a roadmap for recovery through neuroplasticity and education.
- Transition from the frustration of "normal" scans to a proactive management plan that prioritises function and long-term well-being.
Why Talking to Doctors About MUS Often Feels Like a Dead End
For many, talking to doctors about MUS is an exercise in profound frustration. Statistics from 2026 indicate that Medically Unexplained Symptoms account for approximately 45% of all general practice consultations, yet the traditional biomedical model remains ill-equipped to handle them. This model operates like a mechanic looking for a dent in a car’s bodywork. If the "hardware" looks intact on a scan, the system concludes there's no problem. This creates a painful disconnect between clinical data and your lived reality.
When a doctor delivers "normal" test results, they expect you to feel relief. Instead, you likely feel rejected. Without a clear label, your symptoms lack legitimacy in the eyes of the medical system. This often leads to the "all in your head" stigma, a form of medical gaslighting that suggests if a machine can't see the pain, the mind must be inventing it. Validating your physical experience is the first step toward recovery. Your symptoms are real; the current diagnostic tools simply aren't designed to measure the specific way your nervous system is functioning. We believe in diagnosis, not dismissal.
The Gap Between Scans and Sensation
A clear MRI or blood panel doesn't mean your dizziness or chronic pain is absent. It simply confirms the absence of structural damage. In the context of Medically Unexplained Symptoms, it's more helpful to view the body through a "software" lens. While your hardware is sound, the processing of signals between your brain and body has become sensitised. If you spend years searching for a structural "smoking gun," you miss the opportunity to address these functional errors. This delay often allows symptoms to become more entrenched, as the brain's neural pathways for pain become more efficient at sending distress signals.
The 10-Minute Consultation Barrier
The reality of the UK healthcare system is built on the 10-minute appointment. Within this tiny window, GPs are trained to screen for "red flags" such as cancer or organ failure. When these are ruled out, the clinician often defaults to "watchful waiting," a passive approach that leaves patients in limbo. This isn't a personal failing of the doctor, but a limitation of the clinical centre's structure. To break this cycle, you must learn to present your symptoms in a way that fits the system’s logic whilst demanding a focus on your functional quality of life. Shifting your approach is the only way to move from being "undiagnosed" to being heard.
Shifting the Narrative: From Structural Damage to Functional Connection
The traditional medical system often forces a choice between two rigid categories: physical illness or mental health. This binary is not only outdated but clinically inaccurate for those living with persistent symptoms. When you are talking to doctors about MUS, the conversation often stalls because the system is looking for structural damage, like a broken bone or a tumour. However, the reality of your experience lies in the mind-body connection, where the nervous system acts as a high-speed bridge between your internal environment and your physical sensations.
Central sensitisation is the mechanism that explains why you feel real, physical pain despite clear scans. Think of it as the body’s alarm system becoming over-sensitive. The "volume" of your physical signals has been turned up. Whilst there is no "hardware" damage, the "software" is sending constant distress messages. This is not a psychological invention; it is a physiological reality of a nervous system under pressure. Recognising this shift from structure to function is essential for moving toward recovery.
Understanding the Biopsychosocial Lens
To move forward, we must adopt a wider view of health. The biopsychosocial model is a holistic, evidence-based framework that considers the complex interplay between biological, psychological, and social factors in your health. It acknowledges that your symptoms aren't just about cells and chemistry, but also about your history, your environment, and your stress levels. For a deeper dive into this approach, explore our guide on The Mind and Body Connection: A Clinical Guide to Functional Health.
Why "Unexplained" is a Limitation of Science, Not You
The term "unexplained" is a reflection of the current limitations of medical technology, not a reflection of your character or the validity of your pain. We should reframe these symptoms as "functional," meaning they relate to how the body operates amongst daily stressors rather than how it looks on a slide. When talking to doctors about MUS, shifting the focus from "What is the diagnosis?" to "How do I recover?" creates a collaborative atmosphere. This allows you and your clinician to look at the tools needed to regulate the nervous system. If you are looking for practical ways to start this journey, you can explore our resources on functional recovery and neuroplasticity.
How to Organise Your Appointment for Maximum Impact
Preparation, not panic, is the foundation of a successful consultation. In the high-pressure environment of a modern GP surgery, you often have fewer than 600 seconds to convey years of physical distress. When talking to doctors about MUS, your goal is to present a narrative that is clinical, clear, and focused on function. Without a structured plan, the conversation can easily drift into the "dismissal trap," where a lack of structural damage is mistaken for a lack of physical reality. You must lead with evidence, not just emotion.
To avoid being overwhelmed, you should prioritise your symptoms. Trying to cover ten different pains in one session often leads to clinician fatigue and superficial advice. Instead, identify your two most debilitating symptoms. These are the ones that most significantly restrict your daily behaviour or prevent you from working. By narrowing the focus, you help the clinician look for patterns rather than isolated anomalies. Experts at Harvard Health offer valuable guidance on navigating unexplained symptoms, suggesting that a collaborative partnership is more effective than an adversarial one.
Creating a Functional Symptom Map
A symptom map is a tool that translates your internal experience into clinical data. Rather than a simple list, organise your symptoms by frequency, intensity, and their specific impact on your life. Note whether your dizziness peaks after social interactions or if your chronic pain fluctuates based on sleep patterns. This approach highlights the Mind and Body Connection whilst providing the clinician with the "functional" clues they need to move beyond standard red-flag screening. It moves the dialogue from "where does it hurt?" to "how is your body functioning?"
The Pre-Appointment Checklist
Clarity comes from structure. Before you enter the consultation room, ensure you have a concise, chronological history of your symptoms. This prevents the confusion that often arises when trying to remember dates under pressure. Your checklist should include:
- Your top three specific questions regarding symptom management.
- A list of current medications and their observed effects on your function.
- A brief summary of how your symptoms have progressed over the last six months.
Taking this level of control over the 10-minute window ensures your concerns are addressed systematically. For those looking to support their recovery between appointments, our guide on Mind-Body Balance Tools: A Roundup for Functional Symptom Recovery provides practical resources to help regulate your nervous system and build resilience.
Practical Communication Strategies: Using the Biopsychosocial Script
The power dynamic of the consultation room often discourages patients from leading the narrative. When talking to doctors about MUS, the fear of being labelled a "difficult" patient or a "hypochondriac" is real. To bypass this, you must adopt the language of the clinician. Using "functional" terminology allows you to describe your symptoms as a physiological process rather than a psychological mystery. This isn't about self-diagnosis via the internet; it's about providing a clear, evidence-based account of how your body is operating under pressure. We advocate for a stance of "Hope, not hype," where you remain optimistic about recovery whilst grounded in the reality of your physical distress.
The "Mind-Body" Script for Patients
A successful script acknowledges the clinical data whilst insisting on the reality of the sensation. You can lead the conversation by saying: "I recognise that my scans and blood tests are clear, which is reassuring, but my physical experience suggests my nervous system is stuck in an overactive state." This pivot moves the conversation from a negative test result to a functional discussion about regulation. When describing your symptoms, focus on how they limit your behaviour. Instead of saying the pain is a "nine out of ten," explain that the pain prevents you from walking to the local shop or concentrating for more than twenty minutes. This provides the doctor with measurable data they can use to track your progress.
Handling the "It’s Just Stress" Response
When a doctor suggests "it's just stress," they are often trying to apply a biopsychosocial lens but doing so clumsily. Instead of rejecting the idea, validate the doctor's point whilst asking for deeper exploration. You might respond: "I agree that stress is a biological factor amongst my other symptoms, but I need specific guidance on how to lower this physical sensitivity." This approach maintains a collaborative atmosphere whilst ensuring your physical pain isn't dismissed as purely emotional.
If the consultation reaches a stalemate, be assertive. You have the right to ask for "Diagnosis, not dismissal." If your GP is unsure how to proceed, request a referral to a specialist or a clinic that understands functional neurological disorders. These clinicians are trained to look at the connection between the brain and the body without the "all in your head" stigma. To develop the confidence and vocabulary needed for these vital interactions, enrol in our Mind and Body Connection online course.
Moving from Diagnosis to Recovery: The Power of Mind-Body Education
Success in the consultation room is only the beginning of your journey. Once you've navigated the complexities of talking to doctors about MUS, the real work of recovery happens through education and physiological retraining. Understanding the neuroscience behind your symptoms is not just an intellectual exercise; it's a therapeutic intervention. When you learn how the brain processes pain and distress signals, you begin to deactivate the high-alert state that keeps your nervous system in a loop of central sensitisation. This shift moves you from being a passive recipient of medical tests to an active participant in your own healing process.
Neuroplasticity is the cornerstone of this transition. Just as the brain can "learn" to produce chronic pain or dizziness through repetitive signalling, it can also be retrained to prioritise safety over threat. This isn't a quick fix, but a methodical process of rewiring neural pathways. By consistently applying evidence-based tools, you can lower the physical sensitivity of your body. We focus on "Hope, not hype," providing a realistic framework that respects the complexity of the mind-body connection whilst offering a clear path out of the "undiagnosed" state.
Education as a Clinical Tool
Knowledge acts as a biological buffer. When you understand that your symptoms are functional rather than structural, your brain's "threat detection" system begins to settle. Traditional treatments often fail because they address the symptom in isolation without acknowledging the biopsychosocial foundation of the distress. Evidence-based guidance helps reduce health-related anxiety, which is a primary driver of symptom amplification. By lowering the psychological pressure on your system, you create the internal conditions necessary for physical relief to occur. This educational approach aligns with the 2026 trend towards patient-centred care, where understanding is viewed as the first step of treatment.
Your Recovery Roadmap
Recovery requires a structured approach to behaviour change. Start by setting small, achievable goals that focus on function rather than the total absence of pain. This might mean increasing your daily activity by 5% each week or practicing nervous system regulation techniques twice a day. You don't have to navigate this path alone. Joining a community of others with similar functional experiences provides the validation that the traditional medical system often lacks. If you're ready to take the next step and move beyond the frustration of your last appointment, explore the Undiagnosed book and online course to start your recovery journey. We provide the resources you need to move from dismissal to discovery, ensuring your body is finally heard.
Empowering Your Path to Functional Health
Mastering the art of talking to doctors about MUS is the first step in reclaiming your narrative from a medical system that often prioritises structural damage over functional reality. By shifting your focus from "what is broken" to "how do I function," you transform the consultation into a collaborative partnership. We've explored how a clear symptom map and the biopsychosocial script can turn a brief appointment into a meaningful breakthrough. Your symptoms aren't an enigma; they're a signal from a nervous system seeking regulation.
Founded by Dr Csaba Dioszeghy, a Consultant Physician, Undiagnosed offers an evidence-based biopsychosocial approach to help you move beyond dismissal. We provide practical tools for functional symptom management that standard primary care often lacks. It's time to trade the exhaustion of "unexplained" labels for the clarity of neuroplasticity and recovery. Begin your journey to recovery with the Undiagnosed book and online course. You are the expert on your own experience. With the right framework, you can bridge the gap between your mind and body to find lasting relief.
Frequently Asked Questions
What should I do if my doctor says my symptoms are "all in my head"?
If your clinician suggests symptoms are purely psychological, pivot the conversation toward the functional reality of your nervous system. Your pain is real; it's the result of a sensitised nervous system rather than an active imagination. Ask for a discussion on central sensitisation to bridge the gap between their clear scans and your physical experience. This approach ensures you're seeking diagnosis, not dismissal.
Can stress really cause severe physical symptoms like seizures or paralysis?
Stress can indeed manifest as profound physical dysfunction, including non-epileptic seizures or functional limb weakness. When the nervous system is overwhelmed, the brain's "software" can glitch, leading to symptoms that mimic structural damage. These are often categorised as functional symptoms, where the body's hardware is intact but the signals are disrupted by chronic physiological pressure or trauma.
How do I ask for a second opinion regarding my unexplained symptoms?
You have a right to request a second opinion if you feel your current management plan is stagnant or your concerns are being overlooked. Frame the request as a desire for a fresh clinical perspective rather than a criticism of your current GP. State clearly that you'd like to see a clinician with a specific interest in persistent physical symptoms to ensure all functional avenues are explored.
What is the difference between MUS and a Functional Neurological Disorder (FND)?
Medically Unexplained Symptoms (MUS) is a broad umbrella term used when clinical tests don't reveal a structural cause. Functional Neurological Disorder (FND) is a specific diagnosis where the brain and body have trouble sending and receiving signals correctly. Whilst MUS describes a state of being undiagnosed, FND recognises a specific mechanism of nervous system dysfunction that requires targeted neuroplasticity-based recovery.
Is it helpful to bring a friend or family member to my appointment?
Bringing a trusted advocate is highly beneficial for talking to doctors about MUS. They can take notes, help you remember your prepared questions, and provide a witness to the impact of symptoms on your daily behaviour. A companion helps lower your stress levels during the consultation, which makes it easier to communicate your needs clearly and avoid a sense of dismissal.
Why does my doctor keep ordering the same blood tests when they always come back normal?
Doctors repeat tests to ensure no new biological markers have emerged since your last visit. In approximately 10% of cases, initial symptoms that appear unexplained may eventually reveal a structural cause as the condition develops. However, if tests remain consistently normal, it's a signal to shift the focus from ruling out "hardware" damage to managing the "software" of your mind-body connection.
What are the best questions to ask my GP during a 10-minute consultation?
Focus on three specific questions: "What functional mechanisms could explain these sensations?", "What are the next steps for symptom management?", and "Can we look at a biopsychosocial approach for my recovery?". These questions move the dialogue away from diagnostic dead ends and toward practical tools for improvement. They help the clinician see you as an active partner in your health journey.
Can I recover from MUS if I have had symptoms for many years?
Recovery is entirely possible even after decades of symptoms because the brain remains plastic throughout life. Neuroplasticity allows you to retrain sensitised neural pathways at any age. Whilst long-term symptoms may take more time to regulate, the evidence-based principles of mind-body education remain effective for reducing physical distress and improving your functional quality of life regardless of the duration.


